Disclaimer: I transparently state that I did not use Large Language Models to generate the following article. I exclusively used Grammarly software to edit the article and used only my academic research capacity, understanding of the topic and seven years of experience working with athletes in their transition back to their sports. If you see that you can contribute to the article by commenting or arguing a better approach please send an email to:
rzakazimov@birkensports.com
Abstract
Despite the prevalence of costochondritis, there is a lack of consensus on its etiology, diagnosis, and management. While working with six athletes only in 2023 on this syndrome, I did extensive research but was not able to find a training approach or an exercise protocol to alleviate the syndrome completely.
The literature is also skewed toward the elderly population and predominantly female patients. However, in my personal work situation, I dealt with highly active athletes who used to train resistance training, conditioning up to 12 hours per week. I work as a medical training expert to help athletes transition back to their sports and improve their performance.
One athlete trained in JiuJitsu (I), three athletes trained in CrossFit (II, III, IV) and two athletes (V, VI) involved in Olympic weightlifting sports. In 2024 I started to work with a CrossFit athlete in her 30s (VII) who also experienced costochondritis syndrome in 2022 January spanning over two years. I am currently working on this case.
This article primarily aims to provide exercise treatment modalities. Using exercise treatment and breathing work, I was able to completely remove the costochondritis hallmarks among 4 athletes in 2023, significantly decreasing its impact on daily life and training in one athlete unfortunately did not help one client who later the athlete attended other treatment strategies.
Besides training protocols, another important part of medical training is identifying counter-indications that can lead to further damage to deep tissues and increase the magnitude of adhesive tissue in the inflamed regions. Therefore, all clients need to comply with the list of movements and exercises that they can perform. General nutritional guidelines were part of the treatment to decrease the inflammation.
Breaking Injury Cycle:
Before the introduction of the treatment strategies, I always consider the injury cycle. The different stages and circumstances of the problem require specific approaches to deal with. However, independent from treatment strategies, physical exercise and medical training are central to avoiding injury proliferation and increasing sensibility.

General Overview of Treatment Strategies:
The management of Costochondritis syndrome hinges upon a multi-faceted approach tailored to the individual needs and preferences of the patient. Conservative measures, including rest, activity modification, and pharmacotherapy with non-steroidal anti-inflammatory drugs (NSAIDs), constitute the cornerstone of initial management. However, for refractory cases or those necessitating expedited relief, interventional modalities such as localised corticosteroid injections or nerve blocks offer a viable alternative. Emerging therapies, ranging from platelet-rich plasma (PRP) injections to acupuncture, hold promise in expanding the therapeutic armamentarium against costochondritis syndrome, albeit warranting further validation through robust clinical trials.
NOTE: The hallmark of this syndrome lies in its propensity to incite chest pain and tenderness, often mimicking more cardiac pathologies.
However, in my practice of medical training, I focus on the understanding of the two aspects that may lead to the emergence of the syndrome at first place, but not limited: thoracic spine and the pectoralis minor. However, the practice is not limited to these areas. Later in this article I will introduce the training plan.
Mechanical Implications of Thoracic Spine Stiffness:
The thoracic spine, comprising twelve vertebrae, plays a pivotal role in maintaining the structural integrity and dynamic functionality of the rib cage. Optimal thoracic spine mobility is essential for facilitating respiratory excursion, thoracic extension, and rotational movements. However, aberrations in thoracic spine mobility, often manifesting as stiffness or hypomobility, can engender a cascade of bio-mechanical alterations with far-reaching implications.
Specifically, if active population use imbalance training protocols they can induce excessive stiffness in their thoracic spine. With big three liftings - Squat, Bench Press and Deadlifts can potentially reduce the thoracic mobility if the proper training protocol was not followed.
In all 7 cases that I tested athletes thoracic spine with Meloq Devices - I used the method developed by Katherine D. Johnson, MEd, ATC1 and Terry L. Grindstaff to benchmark the range of motion in thoracic spine.
NOTE: In five cases from seven the limitation in thoracic rotation in one side was overlapped with the emergence of inflammation in the similar side. By improving Thoracic spine through the exercise protocols, we gained a significant pain-free range of motion among athletes.
In general, the limitations of the thoracic spine will lead the poor axial rotation which is an important physiological movement of the spine and vitally important in many functional and sporting activities such as gymnastics, boxing, and rowing. Approximately 80% of axial rotation originates in the thoracic spine. Limited thoracic mobility may impair functional performance or predispose individuals to injury in anatomically related regions such as the lower back, neck, or shoulder. So by working on thoracic spine we are not only considering the syndrome by also facilitating a healthy comeback to sports especially in the case of Jiu-Jitsu athlete.
Impact on Costochondral Junctions:
Excessive stiffness in the thoracic spine may disrupt the harmonious interplay between the ribs, sternum, and associated cartilaginous structures, thereby predisposing the costochondral junctions to undue stress and microtrauma. This biomechanical imbalance can lead to localised inflammation and irritation, culminating in the characteristic chest pain and tenderness observed in costochondritis syndrome. Furthermore, restricted thoracic spine mobility may compromise the compensatory mechanisms employed during respiratory efforts, exacerbating the strain on the costochondral junctions and perpetuating the cycle of inflammation.
With the work on Thoracic spine, we also introduced the synergic breath work and increased the time under tension accompanied with long inhale and exhale periods. This training strategy was positively associated with the significant decrease of the pain but did not completely remove the syndrome.
Role of Pectoralis Minor Dysfunction:
The pectoralis minor, a small yet influential muscle situated in the anterior aspect of the chest, serves as a key player in scapular stabilisation and thoracic mobility. Dysfunction or hypertonicity of the pectoralis minor can impart deleterious effects on thoracic spine mobility, accentuating existing stiffness and predisposing to bio-mechanical aberrations. Moreover, the pectoralis minor exerts its influence on the costochondral junctions through its attachments to the ribs, further exacerbating the strain and predisposing to inflammatory changes.

When we observe the structure of the pectoralis minor the problem becomes an evident - athletes that do big three liftings (bench press, squat, deadlift) tend to increase the stiffness in the chest muscles that can create a whole range of problems one being costochondral inflammation.
The stiffness will create an excessive burden on the muscle attachment to the sternum leading to the general aberrations of the range of motion in the anterior field. Therefore the training protocols have to consider the pectoralis minor by progressively introducing exercises where the rib cage movement is relatively stabilised but the pectoralis minor still engages in its muscle function. The functions of the pec minor are stabilization, depression, abduction or protraction, internal rotation and downward rotation of the scapula.
NOTE: It is crucial to mention that similar to the stiffness hyper-mobility [opposite of hypo-mobility] also can lead to the problem. However, in my case of working with athletes they exclusively dealt with stiffness rather than hyper-mobility.
Beyond Thoracic Mobility and Pectoralis Minor:
Although the program will primarily focus on two regions to remove or reduce the impact of the costochondritis however the 4-5 months raining protocols will include several key regions to train. The following table shows exact systematic approach towards the upper body mobilization and reducing the effect of costochondritis.
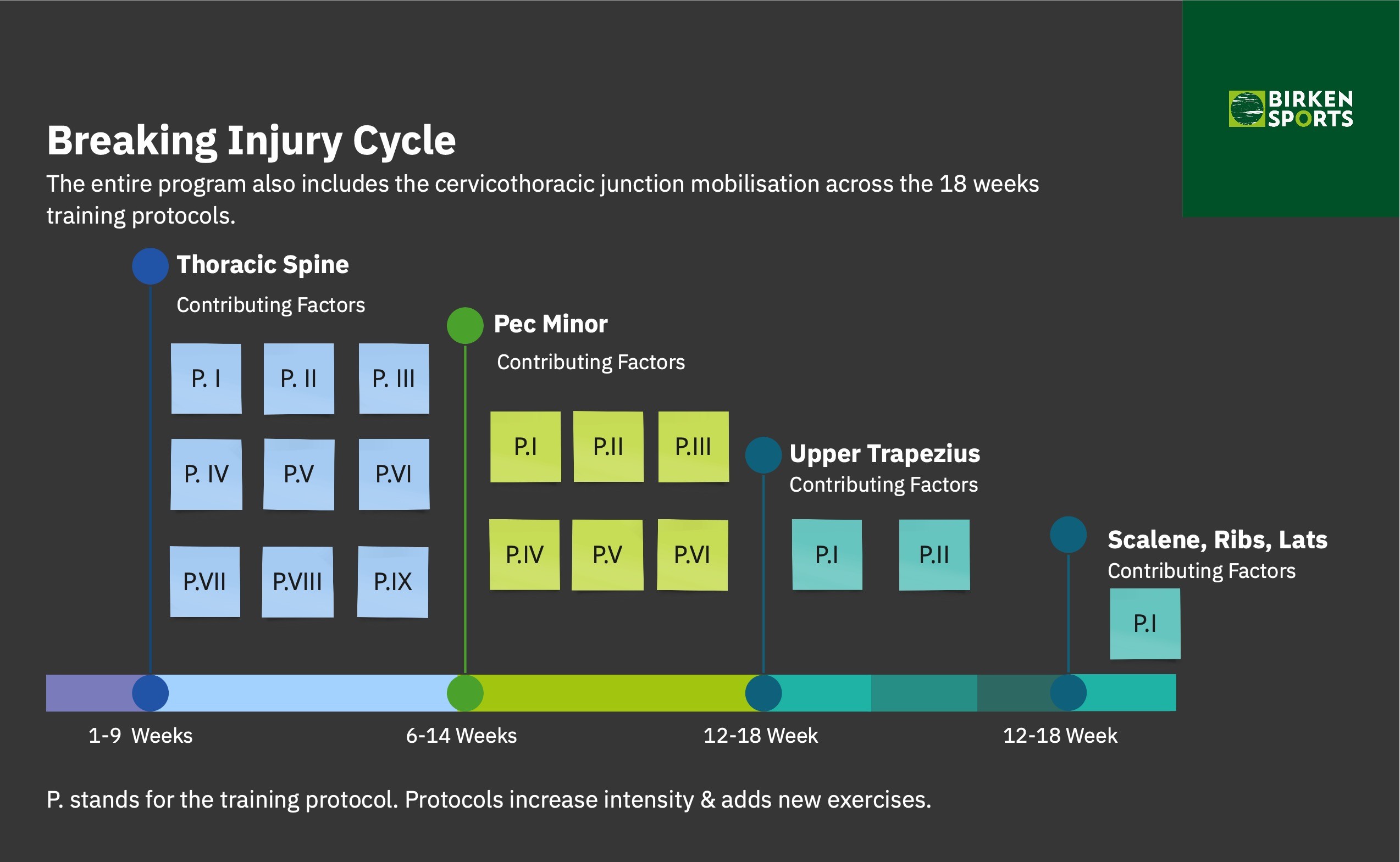
The protocols make sure that I worked with every single contributing factor to the syndrome, thoracic spine, pec minors and cervicothoracic junction being the focus the entire period of training.
Training Protocols
I establish training protocols in the form of exercise database, providing up to 12 variables in the database including video references for the movement quality, sets and reps, progressive load and the training protocols designed by regions in reference to the above graph, 'Breaking Injury Cycle'. The following protocol represents the Protocol 1 for the first 6 weeks of training.
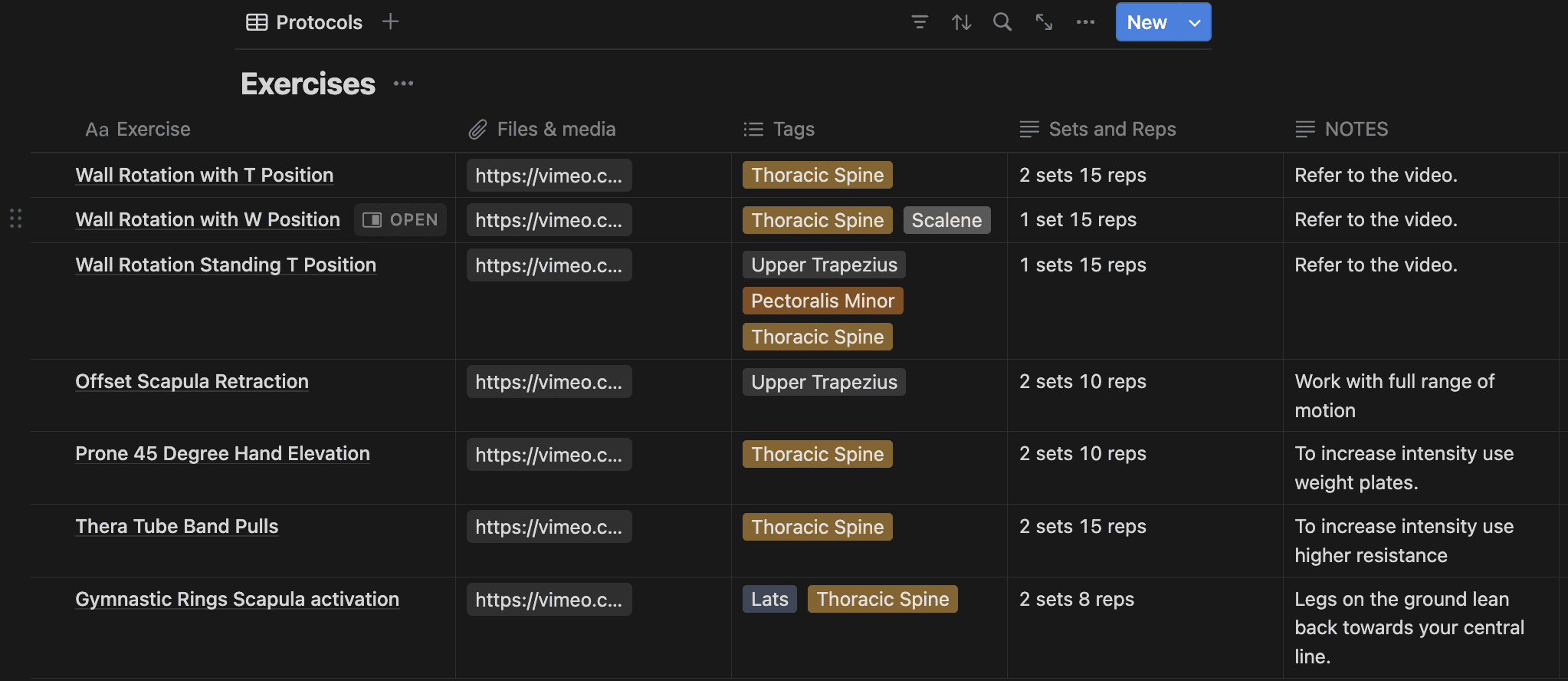
The training modalities are also communicated with athletes to understand the principles of the training system. For example, functional range conditioning and eccentric training are key training modalities that we apply to our training. Finally, we list the counter-indications to avoid further exacerbation of the problem. For example, the bench press is one of the counter-indications that athletes are not allowed to do bench press during the medical training period.
Conclusion
Costochondritis is one of the injury types that necessitated a careful approach to designing training protocols. Athletes need to extensively restore their upper back mobility followed by the pac muscles and other contributing factors. If not treated, costochondritis can lead to multiple different problems increasingly becoming a debilitating factor and limiting athletes' ability to perform a variety of exercises.
In this short article, I established my approach that being successful until now when athletes were not exposed to any alternative treatments other than training. Only one athlete was not able to recover from the injury eventually working with other treatment approaches.



